

Introduction: Mediastinal gray zone lymphoma (MGZL) is an extremely rare form of non-Hodgkin lymphoma with a predominance in young men and with features that are intermediate between nodular sclerosis classical Hodgkin lymphoma (cHL) and primary mediastinal B-cell lymphoma (PMBL). Shared features of these tumor types include tumor CD30 expression and the presence of 9p24.1 chromosomal alterations with expression of programmed death 1 (PD-1) ligand. Compared with PMBL, patients (pts) with MGZL have inferior survival outcomes when treated with conventional chemotherapy (Wilson et al. Blood 2014). Nivolumab is a fully human immunoglobulin G4 anti-PD-1 immune checkpoint inhibitor monoclonal antibody; brentuximab vedotin (BV) is an anti-CD30 antibody-drug conjugate. In the CheckMate 436 study, the combination of nivolumab and BV demonstrated a high objective response rate (ORR; 73%) and complete response (CR) rate (37%) in pts with relapsed/refractory (R/R) PMBL (Zinzani et al. J Clin Oncol 2019). A separate study in R/R cHL also showed impressive efficacy (ORR: 82%; CR: 61%), suggesting some complementary action between the two agents (Herrara et al. Blood 2018). A case series highlighted the clinical activity of PD-1 inhibitor monotherapy in R/R MGZL (Melani et al. N Engl J Med 2017). Given the overlapping features of MGZL with PMBL and cHL, we evaluated the efficacy and safety of nivolumab + BV in a separate MGZL cohort in CheckMate 436.
Methods: The expansion cohort of the open-label, phase 1/2 CheckMate 436 (NCT02581631) study enrolled pts ≥ 18 years old with ECOG performance status of 0 or 1, and with confirmed R/R MGZL after autologous hematopoietic cell transplantation (auto-HCT) or, if ineligible for auto-HCT, after ≥ 2 multi-agent chemotherapy regimens. Pts received 240 mg nivolumab (on Day 8 of Cycle 1, then Day 1 of following cycles) and 1.8 mg/kg BV (on Day 1 of each cycle) every 3 weeks until disease progression or unacceptable toxicity. Primary endpoints were investigator-assessed ORR per the Lugano 2014 criteria and safety. Key secondary endpoints included CR rate, overall survival (OS), duration of response (DOR), and progression-free survival (PFS).
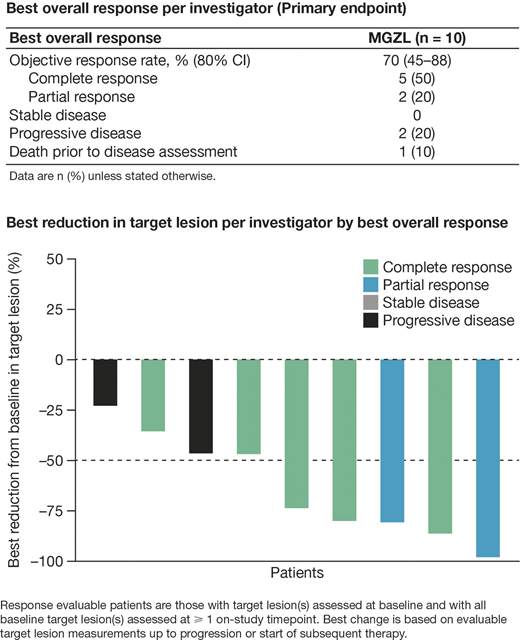
Results: A total of 10 pts were treated and evaluable. Median age (range) was 35 (25-72) years, with only 1 pt aged > 65 years (72 years). Six pts (60%) were male; all pts had a mediastinal mass. Pts had a median of 2 prior lines of systemic cancer therapy, and none had received prior auto-HCT. At database lock, 8 months after the last pt received the first treatment, all pts had discontinued treatment (5 due to disease progression, 3 due to maximum clinical benefit, 1 due to allogenic [allo]-HCT, and 1 due to auto-HCT). Pts received a median of 7 doses of nivolumab and 7 doses of BV. ORR per investigator was 70% (80% CI, 45-88), with 5 pts (50%) achieving CR (Table). The time to CR was 1.2-1.3 months and the duration of CR was 1.5-3.2 months before pts were censored for subsequent therapy. The 5 pts who achieved CR were bridged to hematopoietic cell transplantation (4 allo- and 1 auto-HCT) and censored (all were alive at database lock). Eight pts (89%) who were evaluable for response had tumor reduction of > 25% (Figure). At a median follow-up of 12.4 (range, 0.1-25.5) months, the 6-month OS rate was 80.0% (95% CI, 40.9-94.6). DOR and PFS could not be estimated due to earlier censoring of pts who received subsequent therapies. Nine pts (90%) experienced any grade treatment-related adverse events (TRAEs); the most common any grade TRAEs were neutropenia (n = 3; 1 grade 1, 1 grade 2, 1 experienced 4 grade 1/2 events and 1 grade 3 event) and paresthesia (n = 3; all grade 1). Three pts (30%) had grade 3-4 TRAEs. Infusion-related reaction occurred in 1 pt (grade 1). One pt had an immune-mediated AE (grade 2 maculo-papular rash, which resolved without systemic steroids). A serious drug-related AE occurred in 1 elderly pt (grade 3 febrile neutropenia). There were 3 deaths, all caused by disease progression.
Conclusions: Nivolumab + BV demonstrated a high investigator-assessed ORR of 70%, with a 50% CR rate and a tolerable safety profile in pts with R/R MGZL, similar to findings in PMBL. The regimen represents a potential option for bridging to hematopoietic cell transplantation based on the brisk and frequent responses and a safety profile that compares favorably with historic data using standard chemotherapy regimens.
Study support: BMS. Writing support: Jane Cheung, Caudex, funded by BMS.
Santoro:Takeda, Roche, Abbvie, Amgen, Celgene, AstraZeneca, ArQule, Lilly, Sandoz, Novartis, Bristol-Myers Squibb, Servier, Gilead Sciences, Pfizer, Eisai, Bayer, MSD: Speakers Bureau; Arqule, Sanofi: Consultancy; Bristol Myers Squibb, Servier, Gilead, Pfizer, Eisai, Bayer, MSD: Membership on an entity's Board of Directors or advisory committees; Bristol-Myers Squibb, SERVIER, Gilead Sciences, Pfizer, Eisai, Bayer, MSD, Sanofi, ArQule: Consultancy; Takeda, Roche, Abbvie, Amgen, Celgene, AstraZeneca, ArQule, Lilly, Sandoz, Novartis, Bristol-Myers Squibb, Servier, Gilead Sciences, Pfizer, Eisai, Bayer, MSD: Speakers Bureau; Bristol-Myers Squibb, SERVIER, Gilead Sciences, Pfizer, Eisai, Bayer, MSD, Sanofi, ArQule: Consultancy; Bristol-Myers Squibb, SERVIER, Gilead Sciences, Pfizer, Eisai, Bayer, MSD, Sanofi, ArQule: Consultancy, Speakers Bureau. Moskowitz:Merck: Consultancy; Imbrium Therapeutics, L.P.: Consultancy; Miragen Therapeutics: Consultancy; Incyte: Research Funding; Merck: Research Funding; Bristol-Myers Squibb: Research Funding; Seattle Genetics: Research Funding; Seattle Genetics: Consultancy. Carlo-Stella:Servier, Novartis, Genenta Science srl, ADC Therapeutics, F. Hoffmann-La Roche, Karyopharm, Jazz Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees; Bristol-Myers Squibb, Merck Sharp & Dohme, Janssen Oncology, AstraZeneca: Honoraria; Boehringer Ingelheim and Sanofi: Consultancy; ADC Therapeutics and Rhizen Pharmaceuticals: Research Funding. Fanale:Seattle Genetics: Current Employment, Current equity holder in publicly-traded company. Francis:Bristol-Myers Squibb Company: Current Employment, Current equity holder in publicly-traded company. Sacchi:Bristol-Myers Squibb Company: Current Employment. Savage:Roche (institutional): Research Funding; Merck, BMS, Seattle Genetics, Gilead, AstraZeneca, AbbVie, Servier: Consultancy; BeiGene: Other: Steering Committee; Merck, BMS, Seattle Genetics, Gilead, AstraZeneca, AbbVie: Honoraria.
Nivolumab was used in combination with brentuximab vedotin (BV) for evaluation of its efficacy and safety in patients with relapsed/refractory mediastinal gray zone lymphoma.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal